

Every healthcare organization runs on two parallel systems: the clinical one that treats patients, and the financial one that gets the provider paid for it. Revenue cycle management is the second system — and when it breaks down, even the best clinical care can’t keep the lights on. According to Mordor Intelligence’s 2026 industry analysis, the global revenue cycle management market is valued at roughly US$95.22 billion this year and is projected to climb to US$154.39 billion by 2031, growing at a 10.15% compound annual rate. That growth isn’t happening in a vacuum. It’s a direct response to rising claim denials, more complex payer rules, and providers who are tired of watching earned revenue disappear into administrative gaps. Add in workforce shortages among trained coders and billers, and the pressure on internal teams to keep pace with payer policy changes that shift several times a year, and it’s easy to see why so many organizations are rethinking how they staff and structure this side of the business.
This guide breaks down what revenue cycle management (RCM) actually involves, how the healthcare revenue cycle works stage by stage, what to expect from RCM services, and how to evaluate RCM companies if you’re considering outsourcing. We’ll also cover the technology reshaping medical RCM, the KPIs worth tracking, and the questions practice managers ask most often. Whether you run a two-physician clinic or a multi-site hospital system, the fundamentals of RCM are the same — and getting them right is worth real money.
What Is Revenue Cycle Management in Healthcare?
Revenue cycle management in healthcare is the process providers use to track patient revenue from the first appointment booking through to the final payment received — covering registration, insurance verification, coding, claim submission, payment posting, and collections. In short, it’s the financial lifecycle of a patient encounter, from scheduling to final reimbursement.
Unlike a simple invoicing system, healthcare revenue cycle management has to account for a third party that most other industries don’t deal with at all: the insurance payer. A retail business sells something and gets paid almost immediately. A healthcare provider delivers a service, then waits — sometimes 30, 60, or 90 days — while a payer reviews documentation, applies coverage rules, and decides how much (if any) of the claim it will honor. That waiting period, and everything providers do to shorten and protect it, is what RCM is built to manage.
Here’s the thing — RCM isn’t just a billing department function. It touches front-desk staff collecting insurance cards, clinicians documenting visits in enough detail to support a code, coders translating that documentation into billable language, and finance teams reconciling what actually lands in the bank. When any one of those links is weak, the whole healthcare revenue cycle slows down or leaks money.
It also helps to understand what RCM is not. It isn’t accounting in the traditional sense — a bookkeeper closing monthly ledgers doesn’t touch payer adjudication rules or denial codes. It isn’t pure IT either, even though software runs most of it today. The healthcare revenue cycle sits at the intersection of clinical documentation, insurance contract law, coding standards, and old-fashioned collections — which is exactly why it’s hard to do well and expensive to do badly.
Why the Healthcare Revenue Cycle Matters for Providers
A well-run healthcare revenue cycle isn’t just an accounting nicety. It directly determines whether a practice can hire more staff, invest in new equipment, or simply keep its doors open.
- Cash flow stability. Predictable, faster reimbursement means payroll, supplier payments, and facility costs get covered without scrambling for credit lines.
- Lower administrative cost per claim. A clean, well-managed healthcare revenue cycle reduces the rework, phone calls, and appeals that eat into staff time.
- Better patient experience. Accurate bills sent on time, with clear explanations, reduce confusion and complaints — and patients increasingly judge a provider’s professionalism by how clean the billing experience is, not just the clinical one.
- Regulatory protection. A disciplined RCM process builds in the documentation and compliance checks that protect a provider during a payer audit.
- Strategic planning. Finance leaders can’t forecast hiring, expansion, or equipment purchases with any confidence if the revenue side of the business is unpredictable month to month.
- Audit readiness. Organizations that document eligibility checks, authorizations, and coding decisions consistently spend far less time and money responding to payer audits when they happen.
Honestly, most practices underestimate how much of their actual profit margin lives inside the healthcare revenue cycle rather than the clinical side. Two clinics with identical patient volume and identical fee schedules can post wildly different bottom lines purely because one collects 96% of what it bills and the other collects 84%. That twelve-point gap is rarely a clinical problem. It’s almost always a process problem somewhere inside the revenue cycle. Run the numbers on a mid-sized practice billing $3 million a year, and that twelve-point swing represents roughly $360,000 in revenue that either lands in the bank or quietly disappears into write-offs and unpursued appeals.
Stages of the Healthcare Revenue Cycle
The healthcare revenue cycle is generally broken into three phases — front-end, mid-cycle, and back-end — made up of roughly ten operational stages. Each one feeds the next, so weakness early in the cycle shows up as a financial problem much later.
Front-end (before and during the visit):
- Pre-registration — Collecting demographic and insurance details before the patient arrives, so staff aren’t scrambling at check-in.
- Insurance eligibility verification — Confirming active coverage, benefits, and any prior-authorization requirements in real time, before a single service is delivered.
- Patient registration — Capturing full demographic, contact, and medical history data at check-in, and validating it against what was collected during pre-registration.
- Charge capture — Documenting every billable service, supply, and procedure delivered during the encounter, in language detailed enough to support a code.
Mid-cycle (turning the visit into a claim):
- Medical coding — Translating clinical documentation into standardized ICD-10-CM diagnosis codes and CPT/HCPCS Level II procedure codes, following CMS and AAPC coding guidelines.
- Claim scrubbing — Running the coded claim through an automated check for missing data, mismatched codes, or payer-specific rule violations before it’s ever submitted.
- Claim submission — Sending the scrubbed claim electronically to the payer via EDI for adjudication, then tracking it until a decision comes back.
Back-end (getting paid and staying paid):
- Payment posting — Recording the payer’s reimbursement against the patient account once adjudication is complete, down to the individual claim line.
- Denial management — Investigating, correcting, and appealing any claim the payer rejects or underpays, and feeding the findings back upstream.
- Patient billing and collections — Invoicing the patient for any remaining balance (co-pays, deductibles, non-covered services) and following up on outstanding amounts.
Skip or rush any one of these ten stages and the effects ripple downstream — a missed eligibility check at stage two, for example, almost guarantees a denial at stage nine. Providers who map their own healthcare revenue cycle against these ten stages usually find the weak link within a single afternoon of honest review.
Front-end accuracy tends to pay the largest dividend, dollar for dollar. A clean eligibility check costs a few minutes of staff time. The denial it prevents downstream can cost a coder, a biller, and an AR specialist a combined hour or more once you add up the original submission, the rework, the resubmission, and the follow-up calls. Practices that move even one or two front-end checks from “occasional” to “every single visit” routinely see denial volume drop within a single billing cycle.
Ownership of these stages often splits across departments that rarely talk to each other directly — front-desk staff, clinical documentation teams, coders, and finance — which is part of why handoffs are where most errors creep in. A clear escalation path, where a coder can flag a documentation gap back to the clinician the same day rather than weeks later during an audit, closes that gap faster than any software upgrade ever will. Smaller practices sometimes solve this with a five-minute weekly stand-up between billing and front-desk staff rather than building a formal escalation system from scratch.
Revenue Cycle Management in Medical Billing: How the Two Connect
People often use “medical billing“ and “revenue cycle management” interchangeably, and that’s not quite right. Medical billing is one component — arguably the most visible one — inside the much broader discipline of revenue cycle management in healthcare.
Medical billing specifically covers coding the encounter, generating the claim, and submitting it for payment. RCM in a medical billing context means billing doesn’t operate as a standalone task; it’s wired into eligibility verification upstream and denial management, payment posting, and collections downstream. A biller who codes a claim perfectly but works from a practice that never verifies insurance up front is still going to see denials pile up, no matter how clean the coding was.
This is why CareVanta and most serious RCM companies structure their teams around the full cycle rather than billing alone. A billing-only vendor fixes one link in the chain; a full RCM partner manages the whole chain, which is where the real financial recovery tends to show up. Think of medical billing as the engine and the broader healthcare revenue cycle as the entire vehicle — a great engine in a car with no brakes or steering still won’t get you where you’re going.
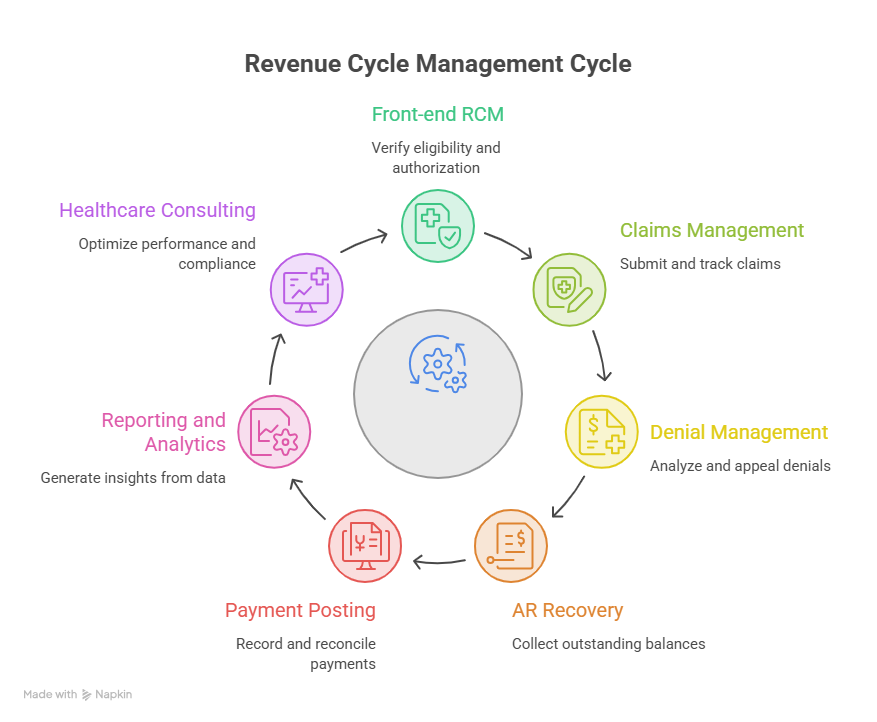
Key Components of Effective Revenue Cycle Management Services
Strong RCM services are built around a handful of core functions, each staffed and measured separately even when delivered by a single vendor.
- Front-end RCM — eligibility verification, authorization tracking, and charge entry, designed to stop errors before they ever reach a claim.
- Claims management — coding support, electronic submission, and active claim tracking through adjudication.
- Denial management — root-cause analysis on denied claims, structured appeals, and workflow fixes so the same denial reason doesn’t keep recurring.
- Accounts receivable (AR) recovery — dedicated follow-up on aging insurance and patient balances, prioritized by dollar value and age.
- Payment posting and reconciliation — accurate, timely recording of every payment against the right account and the right claim line.
- Reporting and analytics — AR aging reports, denial trend dashboards, and collection performance metrics that turn raw billing data into decisions.
- Healthcare consulting — performance benchmarking, workflow optimization, and compliance advisory layered on top of day-to-day operations.
Which brings us to a fair question: do you need all seven, or just one or two? Smaller practices with a tight, well-trained front desk might only need claims management and denial management support. Larger systems juggling multiple payer contracts usually benefit from the full stack, because problems in one component tend to surface as symptoms in another — a denial spike, for instance, often traces back to a front-end eligibility gap nobody flagged as urgent.
Most vendors price these components two ways: bundled, where you pay one fee for the full stack regardless of how much of each service you actually use, or a-la-carte, where you pick specific components and pay only for those. Bundled pricing tends to suit practices that want a single point of accountability. A-la-carte suits practices that already have a strong in-house team and just need help with one weak link, like denial appeals or AR follow-up on aging balances.
In-House vs. Outsourced RCM
This is the decision most practice managers eventually have to make, and there’s no universally “right” answer — only the right answer for a given size, budget, and growth stage.
| Factor | In-House RCM | Outsourced RCM (via RCM Companies) |
| Upfront cost | Higher — salaries, software licenses, training | Lower — typically a percentage of collections or flat fee |
| Staffing risk | High — turnover and coding-skill gaps hit performance directly | Low — vendor absorbs hiring, training, and coverage |
| Scalability | Slow — adding capacity means hiring and onboarding | Fast — vendor reallocates trained staff as volume changes |
| Technology cost | Borne entirely by the practice | Usually included in the service fee |
| Control and visibility | Direct, day-to-day oversight | Indirect — depends on vendor reporting quality |
| Best suited for | Large systems with dedicated finance leadership | Small-to-mid practices, multi-specialty groups, new practices |
Neither model is automatically cheaper once you account for hidden costs — a small in-house team without a certified coder on staff can lose more to denials than an outsourcing fee would have cost. That’s the math worth running before deciding, and it’s one most practices skip until cash flow forces the conversation.
How to Choose the Right Revenue Cycle Management Companies
If outsourcing makes sense, the next step is separating serious RCM companies from vendors that are really just billing services wearing an RCM label.
| Criteria | What to Look For | Why It Matters |
| Specialty experience | Track record in your specific specialty (e.g., DME, home health, ambulance, dental) | Coding and payer rules vary significantly by specialty |
| Technology compatibility | Proven integration with your EHR/PMS system | Poor integration creates duplicate work and data gaps |
| Compliance posture | HIPAA-compliant processes, documented data security practices | Protects you from breach liability and audit exposure |
| Transparency | Real-time dashboards for AR aging, denials, and collections | You should never be guessing where your money is |
| Denial performance | Published or referenceable denial-reduction results | Denial handling is where most revenue actually gets recovered |
| Contract flexibility | No excessive lock-in, clear exit terms | Protects you if the partnership underperforms |
It’s worth noting that pricing shouldn’t be the first filter when comparing RCM companies. A vendor charging slightly more but running a 97% clean-claims rate will out-earn a cheaper vendor running at 88%, every single time, once you do the math on actual dollars collected. Ask any shortlisted vendor for referenceable denial-rate or net-collection-rate improvements from a comparable specialty — not generic marketing claims.
Medical Revenue Cycle Management: Technology and Automation Trends
Medical RCM has shifted hard toward automation over the last few years, and the trend isn’t slowing down.
- Real-time eligibility verification — checking coverage in seconds rather than relying on outdated insurance card data.
- AI-assisted coding — software that suggests ICD-10/CPT codes based on clinical documentation, reducing both coder workload and error rates.
- Automated claim scrubbing — rules engines that catch missing modifiers, mismatched codes, or payer-specific formatting issues before submission.
- Predictive denial analytics — models that flag claims likely to be denied before they’re even sent, based on historical payer behavior.
- Patient engagement platforms — text and portal-based billing that lets patients see, understand, and pay balances without a phone call.
- EHR-integrated reporting — dashboards pulling clinical and financial data into one view, instead of two disconnected systems.
- Robotic process automation (RPA) — bots that handle repetitive, rules-based tasks such as eligibility checks and status lookups, freeing staff for exception handling.
- Interoperability standards — FHIR-based data exchange that lets clearinghouses, payers, and EHRs share claim status without manual phone calls or portal lookups.

What I’ve seen across smaller practices specifically is a reluctance to adopt these tools because they assume automation is built for hospital-scale volume. It isn’t anymore — most modern platforms scale down just as cleanly as they scale up, and the ROI on automated RCM often shows up faster in a smaller, simpler claim volume than in a sprawling hospital system with dozens of legacy integrations to untangle. A ten-physician group automating eligibility checks alone, for example, might save two to three staff hours a day — often enough to redeploy a full-time employee toward AR follow-up instead of routine verification calls.
Data security deserves a mention alongside all this automation. Every one of these tools touches protected health information at some point, whether it’s a clearinghouse passing claim status back and forth or an AI model reading clinical notes to suggest a code. Vendors should be able to explain, in plain language, where that data lives, who can access it, and how long it’s retained — and a practice adopting new software is well within its rights to ask for that explanation before signing anything, not after.
Common Challenges in Healthcare Revenue Cycle Management
Even with better technology, healthcare revenue cycle management still runs into the same recurring obstacles.
- Rising denial rates. Experian Health’s State of Claims 2025 report found that 41% of providers now report denial rates above 10%, up from 38% in 2024 and 30% just three years earlier. That’s not a small drift — it’s a structural shift in how aggressively payers are reviewing claims.
- Coding and billing complexity. Thousands of ICD-10-CM and CPT codes, updated annually, make it easy for even experienced coders to fall behind on changes.
- Payer variability. Every payer has its own cover rules, prior-authorization thresholds, and timely-filing limits, multiplying the number of “correct” claim formats a billing team has to track.
- Growing patient financial responsibility. High-deductible health plans push more of the bill onto patients directly, and patients are statistically harder to collect from than insurers.
- Staff turnover. Roles inside RCM departments see high attrition, and every departure resets institutional knowledge about payer quirks and denial patterns.
- Technology integration gaps. EHRs, billing software, and patient portals that don’t talk to each other create silos that hide problems until AR is already aging.
- Compliance pressure. HIPAA, payer-specific documentation rules, and evolving CMS guidance all carry financial penalties for non-compliance.
- Workforce shortages in coding and billing. Demand for certified coders has outpaced the supply of trained professionals in many regions, pushing salaries up and making vacant positions harder to fill quickly.
- The shift toward value-based contracts. Payment models tied to quality metrics and outcomes, rather than pure service volume, require reporting capabilities that many legacy billing systems weren’t built to handle.
None of these challenges are new exactly — but they’re compounding faster than most internal teams can keep pace with, which is exactly why the outsourced segment of revenue cycle management keeps growing even as automation improves.
Best Practices to Improve RCM Performance
A few habits separate high-performing healthcare revenue cycles from the rest, regardless of whether the work is done in-house or outsourced:
- Verify eligibility before every visit, not just new-patient visits. Coverage changes more often than practices expect.
- Collect patient responsibility estimates up front. Transparent, pre-visit cost conversations reduce bad debt later.
- Scrub every claim before submission. A five-minute automated check prevents a 45-day denial cycle.
- Track denials by reason code, not just by volume. Patterns reveal fixable root causes — a specific modifier error, a specific payer, a specific provider’s documentation habits.
- Set a hard AR aging threshold. Most well-run practices don’t let balances sit past 90 days without an active follow-up plan.
- Train staff on coding updates annually, at minimum. ICD-10-CM and CPT changes happen every year, and stale knowledge is a denial generator.
- Review KPIs monthly, not quarterly. Problems inside the healthcare revenue cycle compound fast; a quarterly review catches them too late.
- Audit a sample of clean claims, not just denials. Reviewing claims that paid correctly often reveals an undercoding that’s quietly leaving money on the table.
- Build patient payment plans into the workflow, not as an afterthought. Offering structured plans up front collects more than chasing a single large balance after the fact.
- Set clear performance SLAs if you outsource. Whether it’s a denial-resolution turnaround time or a claims-submission window, written expectations keep an outsourced partner accountable.
This is often overlooked, but communication between clinical and billing staff matters more than most software vendors will admit. A coder who can walk down the hall and ask a physician to clarify documentation resolves in minutes what would otherwise become a denial three weeks later.
Measuring Success: KPIs for Revenue Cycle Management Healthcare Programs
You can’t improve what you don’t measure. These are the benchmarks practice managers running an RCM healthcare program should track every month:
- Days in Accounts Receivable (Days in AR): Industry best practice generally targets under 40 days. Anything climbing past 50–60 signals a collections problem.
- Net Collection Rate: The percentage of allowed (not billed) revenue actually collected. High-performing practices sit at 95% or above.
- Clean Claims Rate: The percentage of claims accepted on first submission without errors. A strong target is 95–98%.
- Denial Rate: The percentage of claims denied on first submission. Best-in-class practices keep this in the low single digits; the national trend, unfortunately, is moving the other way.
- Cost to Collect: What it costs the practice (in staff time, software, or vendor fees) to collect each dollar of revenue. Lower is better, but not at the expense of denial control.
- First-Pass Resolution Rate: How many claims are fully resolved — paid correctly — without any rework, resubmission, or appeal.
Tracking even three of these consistently — Days in AR, Net Collection Rate, and Denial Rate — gives most practices an early warning system long before cash flow problems become visible on a bank statement. The healthcare revenue cycle rarely fails overnight; it erodes quietly over a few bad months that nobody was watching closely enough.
One caution worth noting: national benchmarks are a starting point, not a finish line. A dermatology practice and a home health agency will see naturally different clean claims rates simply because of how differently their payers handle each specialty. The more useful exercise is tracking your own numbers month over month and asking why a metric moved, rather than chasing an industry average that may not reflect your specific payer mix.
Whoever owns these numbers should report them somewhere visible — a shared dashboard, a monthly one-page summary, a recurring agenda item in a leadership meeting — rather than burying them in a spreadsheet only one person opens. Practices that treat these figures as a quiet back-office exercise tend to notice problems only after they’ve already cost real money, while practices that put the same numbers in front of clinical leadership tend to catch and fix issues within weeks instead of quarters
Final Words
Revenue cycle management in healthcare isn’t a back-office afterthought — it’s the financial engine that determines whether good clinical work actually translates into a sustainable practice. From the first eligibility check to the last collected dollar, every stage of the healthcare revenue cycle either protects revenue or quietly leaks it. Whether you build that capability in-house, partner with established RCM companies, or run a hybrid model, the goal stays the same: faster, cleaner reimbursement with fewer denials and less administrative drag. Providers who treat their healthcare revenue cycle with the same discipline they bring to patient care tend to end up with both — healthier patients and a healthier balance sheet. If you’re evaluating revenue cycle management services for your organization, CareVanta’s RCM team works as an extension of your practice across front-end RCM, claims management, denial management, and reporting, so reach out for a revenue cycle performance assessment tailored to your specialty.
Frequently Asked Questions
What is revenue cycle management in healthcare?
Revenue cycle management in healthcare is the end-to-end financial process providers use to capture, manage, and collect revenue from patient services — spanning registration, insurance verification, coding, claim submission, payment posting, and collections.
What are the main stages of the healthcare revenue cycle?
The healthcare revenue cycle moves through front-end stages (pre-registration, eligibility verification, registration, charge capture), mid-cycle stages (coding, claim scrubbing, submission), and back-end stages (payment posting, denial management, patient billing).
How is revenue cycle management different from medical billing?
Medical billing — coding and submitting claims — is one function inside the broader revenue cycle management process, which also covers eligibility verification, denial management, payment posting, and collections.
What do RCM services typically include?
Most revenue cycle management services cover front-end RCM, claims management, denial management, AR recovery, payment posting and reconciliation, reporting and analytics, and often healthcare consulting on top.
How do I choose the right RCM company?
Evaluate specialty experience, EHR/PMS integration, HIPAA compliance, reporting transparency, proven denial-reduction performance, and contract flexibility — in that order, before price.
What KPIs should healthcare providers track in RCM?
Days in AR, net collection rate, clean claims rate, denial rate, cost to collect, and first-pass resolution rate are the core metrics worth monitoring monthly.
Can small practices benefit from outsourcing revenue cycle management?
Yes — smaller practices often lack the staff depth to absorb turnover or stay current on coding changes, and outsourcing to established revenue cycle management companies can lower denial rates without the fixed cost of an in-house specialist team.