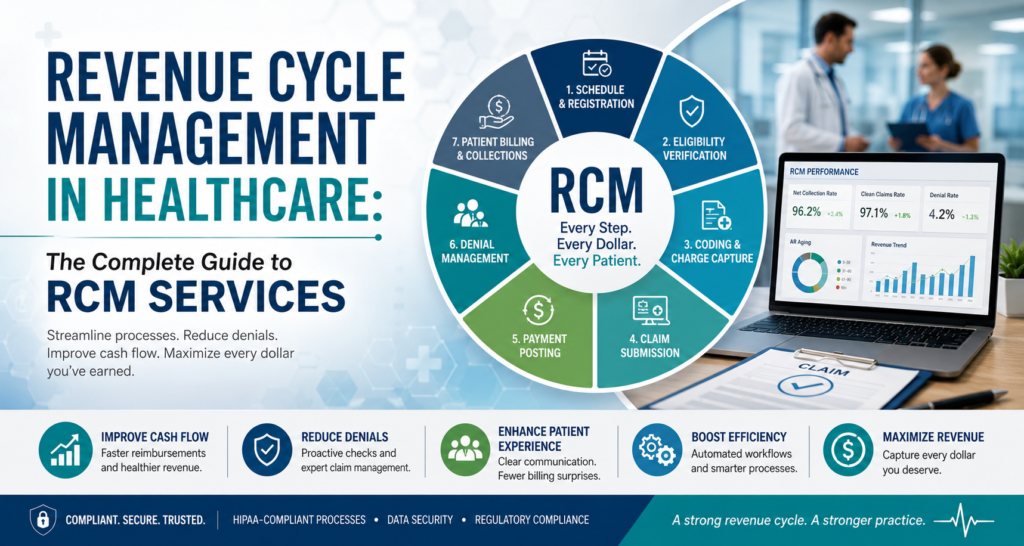
Revenue Cycle Management in Healthcare: The Complete Guide to RCM Services
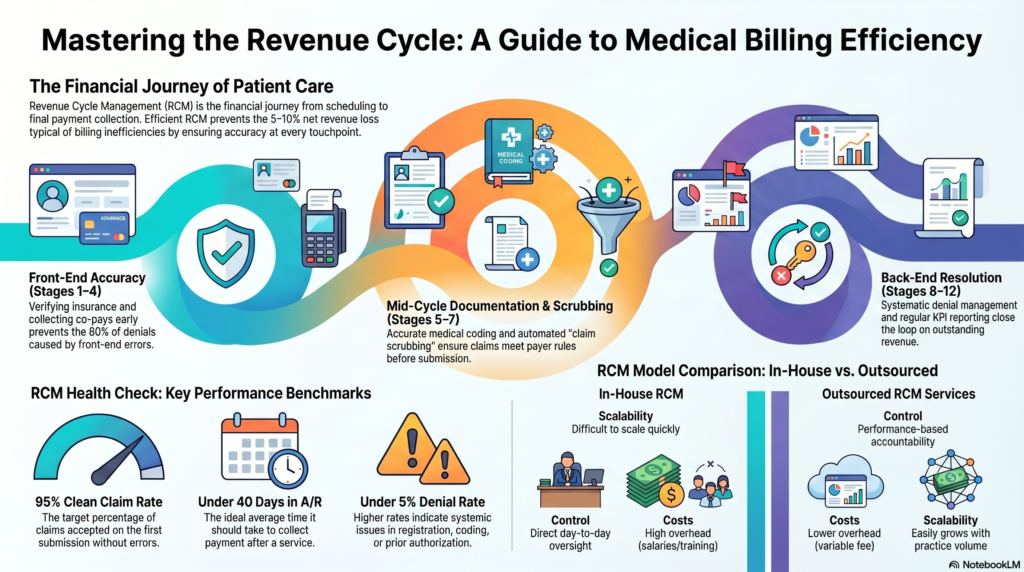
Every healthcare organization runs on two parallel systems: the clinical one that treats patients, and the financial one that gets the provider paid for it. Revenue cycle management is the second system — and when it breaks down, even the best clinical care can’t keep the lights on. According to Mordor Intelligence’s 2026 industry analysis, the global revenue cycle management market is valued at roughly US$95.22 billion this year and is projected to climb to US$154.39 billion by 2031, growing at a 10.15% compound annual rate. That growth isn’t happening in a vacuum. It’s a direct response to rising claim denials, more complex payer rules, and providers who are tired of watching earned revenue disappear into administrative gaps. Add in workforce shortages among trained coders and billers, and the pressure on internal teams to keep pace with payer policy changes that shift several times a year, and it’s easy to see why so many organizations are rethinking how they staff and structure this side of the business. This guide breaks down what revenue cycle management (RCM) actually involves, how the healthcare revenue cycle works stage by stage, what to expect from RCM services, and how to evaluate RCM companies if you’re considering outsourcing. We’ll also cover the technology reshaping medical RCM, the KPIs worth tracking, and the questions practice managers ask most often. Whether you run a two-physician clinic or a multi-site hospital system, the fundamentals of RCM are the same — and getting them right is worth real money. What Is Revenue Cycle Management in Healthcare? Revenue cycle management in healthcare is the process providers use to track patient revenue from the first appointment booking through to the final payment received — covering registration, insurance verification, coding, claim submission, payment posting, and collections. In short, it’s the financial lifecycle of a patient encounter, from scheduling to final reimbursement. Unlike a simple invoicing system, healthcare revenue cycle management has to account for a third party that most other industries don’t deal with at all: the insurance payer. A retail business sells something and gets paid almost immediately. A healthcare provider delivers a service, then waits — sometimes 30, 60, or 90 days — while a payer reviews documentation, applies coverage rules, and decides how much (if any) of the claim it will honor. That waiting period, and everything providers do to shorten and protect it, is what RCM is built to manage. Here’s the thing — RCM isn’t just a billing department function. It touches front-desk staff collecting insurance cards, clinicians documenting visits in enough detail to support a code, coders translating that documentation into billable language, and finance teams reconciling what actually lands in the bank. When any one of those links is weak, the whole healthcare revenue cycle slows down or leaks money. It also helps to understand what RCM is not. It isn’t accounting in the traditional sense — a bookkeeper closing monthly ledgers doesn’t touch payer adjudication rules or denial codes. It isn’t pure IT either, even though software runs most of it today. The healthcare revenue cycle sits at the intersection of clinical documentation, insurance contract law, coding standards, and old-fashioned collections — which is exactly why it’s hard to do well and expensive to do badly. Why the Healthcare Revenue Cycle Matters for Providers A well-run healthcare revenue cycle isn’t just an accounting nicety. It directly determines whether a practice can hire more staff, invest in new equipment, or simply keep its doors open. Honestly, most practices underestimate how much of their actual profit margin lives inside the healthcare revenue cycle rather than the clinical side. Two clinics with identical patient volume and identical fee schedules can post wildly different bottom lines purely because one collects 96% of what it bills and the other collects 84%. That twelve-point gap is rarely a clinical problem. It’s almost always a process problem somewhere inside the revenue cycle. Run the numbers on a mid-sized practice billing $3 million a year, and that twelve-point swing represents roughly $360,000 in revenue that either lands in the bank or quietly disappears into write-offs and unpursued appeals. Stages of the Healthcare Revenue Cycle The healthcare revenue cycle is generally broken into three phases — front-end, mid-cycle, and back-end — made up of roughly ten operational stages. Each one feeds the next, so weakness early in the cycle shows up as a financial problem much later. Front-end (before and during the visit): Mid-cycle (turning the visit into a claim): Back-end (getting paid and staying paid): Skip or rush any one of these ten stages and the effects ripple downstream — a missed eligibility check at stage two, for example, almost guarantees a denial at stage nine. Providers who map their own healthcare revenue cycle against these ten stages usually find the weak link within a single afternoon of honest review. Front-end accuracy tends to pay the largest dividend, dollar for dollar. A clean eligibility check costs a few minutes of staff time. The denial it prevents downstream can cost a coder, a biller, and an AR specialist a combined hour or more once you add up the original submission, the rework, the resubmission, and the follow-up calls. Practices that move even one or two front-end checks from “occasional” to “every single visit” routinely see denial volume drop within a single billing cycle. Ownership of these stages often splits across departments that rarely talk to each other directly — front-desk staff, clinical documentation teams, coders, and finance — which is part of why handoffs are where most errors creep in. A clear escalation path, where a coder can flag a documentation gap back to the clinician the same day rather than weeks later during an audit, closes that gap faster than any software upgrade ever will. Smaller practices sometimes solve this with a five-minute weekly stand-up between billing and front-desk staff rather than building a formal escalation system from scratch. Revenue Cycle Management in Medical Billing: How the Two Connect People often